


Treat an enlarged prostate without surgery.
PAE is a minimally invasive, image-guided procedure that shrinks an enlarged prostate (BPH) to relieve urinary symptoms — no cutting, no general anesthesia, and a much lower risk of sexual side effects than TURP. Performed as an outpatient by a board-certified interventional radiologist.
PAE at a glance
A non-surgical, image-guided procedure — typically 1–2 hours, home the same day.
Symptom improvement in studies
Typical prostate volume reduction
Local anesthesia & light sedation
Image-guided procedures by our physician
Quick Answer
Prostate artery embolization (PAE) is a minimally invasive treatment for an enlarged prostate (BPH). Instead of cutting or removing prostate tissue, an interventional radiologist guides a thin catheter to the prostate arteries and injects tiny particles to reduce its blood supply, shrinking the gland and easing urinary symptoms. Studies report 75–85% symptom improvement, it’s done as an outpatient under local anesthesia, and it carries a much lower risk of sexual side effects than TURP.
Needle puncture, no cutting
Home the same day
Symptom improvement
Preserves sexual function
PAE is only as good as the hands performing it
The prostate arteries are small, variable, and tucked among other pelvic vessels — so PAE rewards an operator with deep embolization experience and exceptional catheter skill. That's the core of what we do.
Dr. Atabak Allaei was among the early adopters of PAE and has helped advance non-surgical treatment for enlarged prostate. He is the Medical Director of California Vascular & Interventional and serves on staff at Cedars-Sinai Medical Center and UCI Health. Crucially, this is a primary embolization practice — not an occasional add-on — which is exactly the background that makes PAE safer and more effective, especially in challenging anatomy.
Among the first to perform PAE
An early adopter of prostate artery embolization who helped advance the non-surgical option — years of focused PAE experience, not a recent addition to the menu.
A primary embolization practice
Embolization is the focus here — prostate, fibroid, musculoskeletal, and tumor work across the lungs, liver, kidneys, pelvis, and vascular system. 5,000+ image-guided procedures in total.
Superior catheter & wire skill
PAE depends on precise navigation through tiny, tortuous arteries. A background in complex embolization translates directly into the catheter and wire control that makes the procedure successful.
Double board-certified, fellowship-trained
Board-certified in Vascular & Interventional Radiology and Diagnostic Radiology, fellowship-trained at the Mallinckrodt Institute (Washington University / Barnes-Jewish).
More than
More than
Find out in under a minute – no phone call needed.
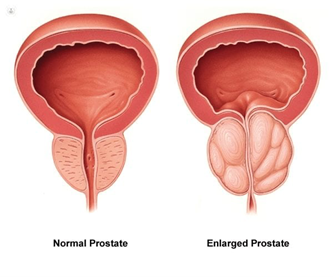
What is an enlarged prostate (BPH)?
Benign prostatic hyperplasia (BPH) is a common, non-cancerous enlargement of the prostate that squeezes the urethra and disrupts urination.
Left untreated, severe BPH can lead to urinary retention, bladder stones, or kidney damage. The good news is that there are many effective options — from lifestyle changes and medication to minimally invasive procedures like PAE and surgery such as TURP.
What are the treatment options for BPH?
Treatment usually starts with lifestyle changes and medication; when those aren't enough, minimally invasive PAE or surgery are considered.
Initial steps often include reducing fluids before bed and limiting bladder irritants like caffeine and alcohol. If symptoms progress, medication is usually next:
- Alpha-blockers (e.g. tamsulosin) relax the bladder-neck and prostate muscles to improve flow.
- 5-alpha-reductase inhibitors (e.g. finasteride) shrink the prostate over time.
- Combination therapy can be especially effective for larger prostates.
- PDE-5 inhibitors (e.g. tadalafil), sometimes used when erectile dysfunction is also a concern.2
What is prostate artery embolization (PAE)?
PAE is a minimally invasive procedure that shrinks the prostate by reducing its blood supply — performed by an interventional radiologist, with no surgical cutting.
Rather than removing or cutting prostate tissue, PAE blocks the small arteries that feed the prostate. With less blood flow, the gland gradually shrinks (a controlled, gentle process), which relieves pressure on the urethra and improves urinary symptoms over the following weeks.3
Because it works through a tiny catheter rather than an incision, PAE has a favorable risk profile and is particularly valuable for men who are poor candidates for surgery or who want to preserve sexual function.
What are the advantages of PAE?
PAE avoids the cutting, anesthesia, and sexual side effects of surgery — while still delivering meaningful, lasting symptom relief.
- Minimally invasive — a needle puncture, not surgical cutting
- No stitches, and no internal cutting, bleeding, or burning
- No general anesthesia — performed under local anesthesia and light sedation
- No risk to the testicular artery or nerve, and no risk of hydrocele
- Outpatient — most men go home the same day
- Quick recovery with fewer activity restrictions than surgery
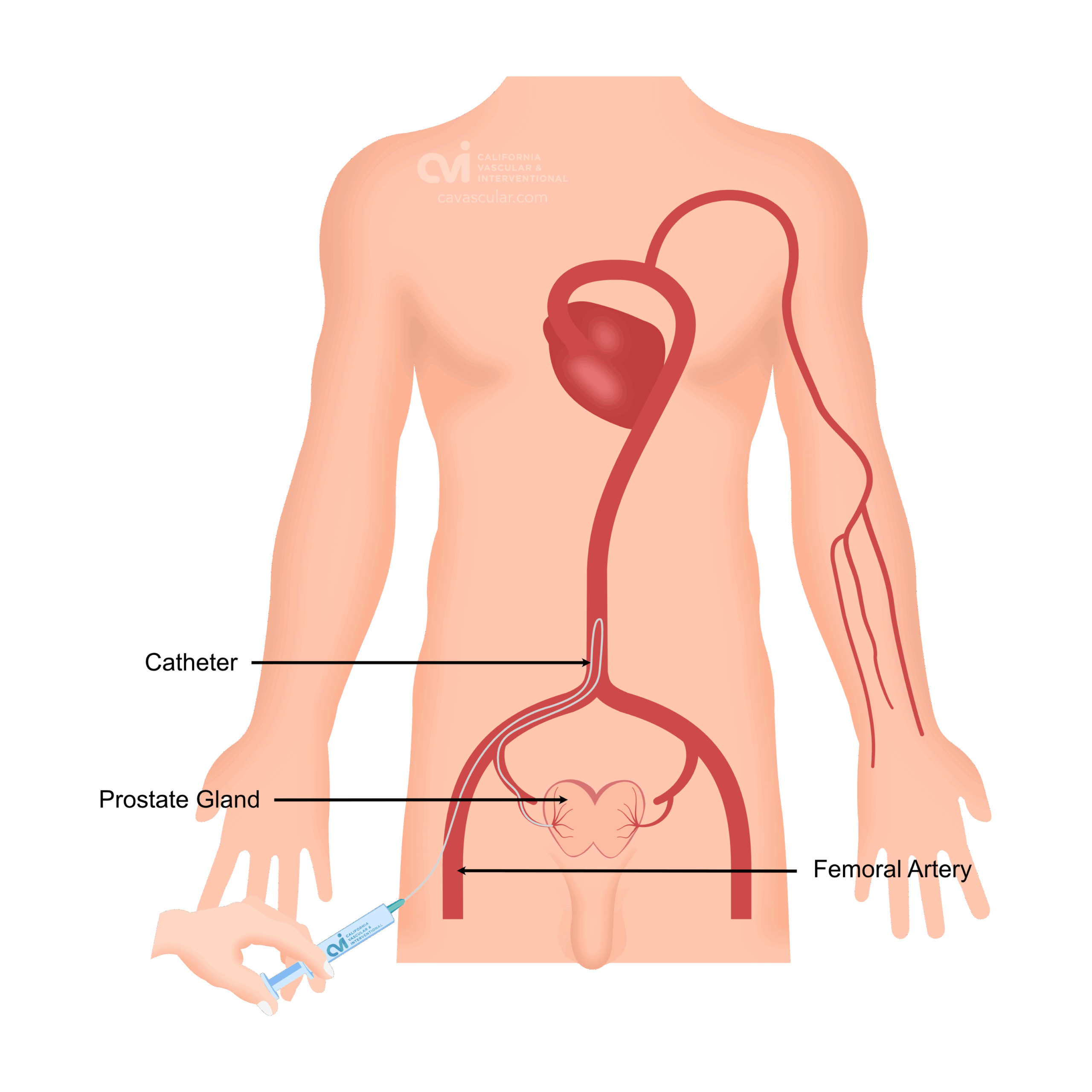
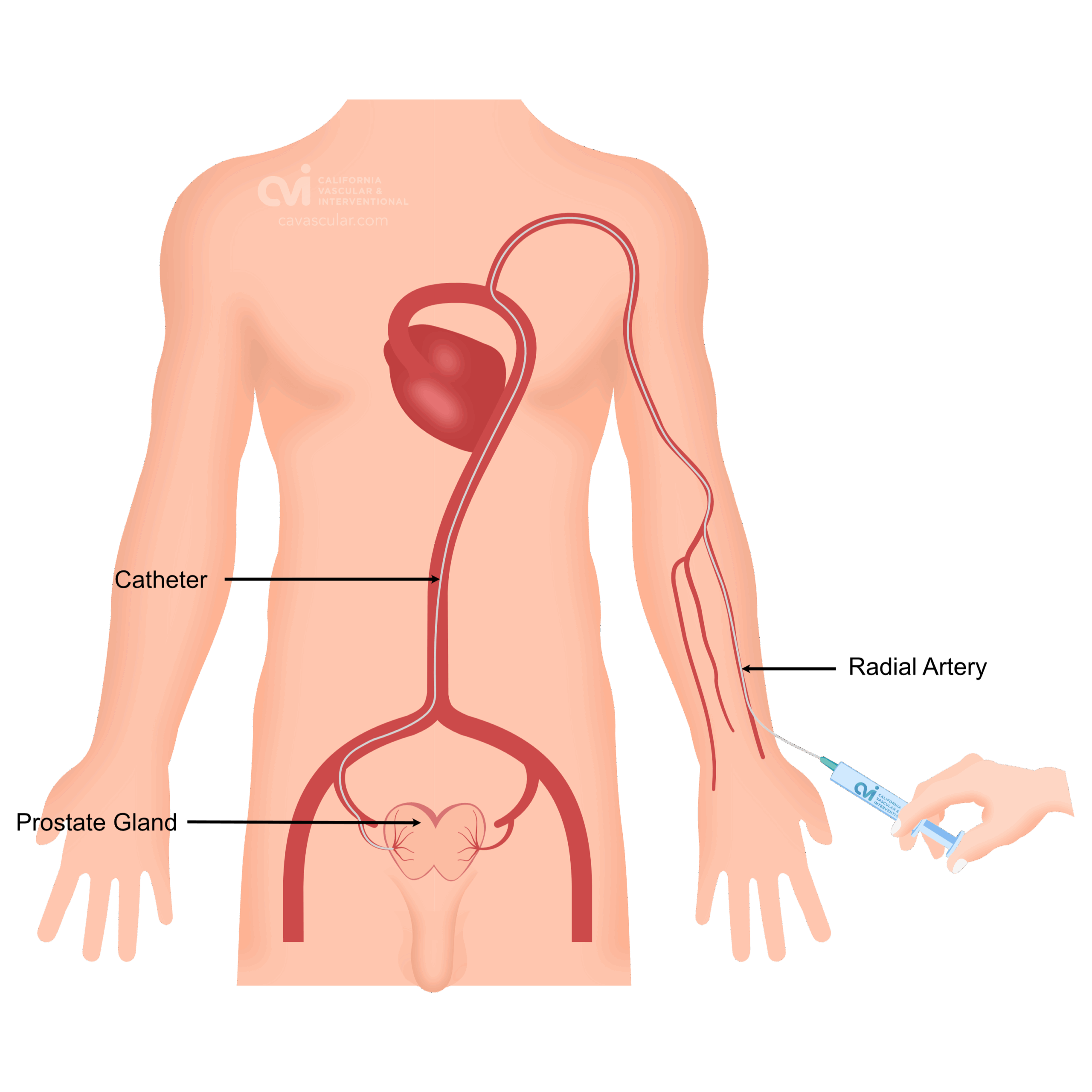
How is prostate artery embolization performed?
The whole procedure usually takes 1–2 hours, under local anesthesia and light sedation, on an outpatient basis.
Local anesthesia & sedation
Catheter access
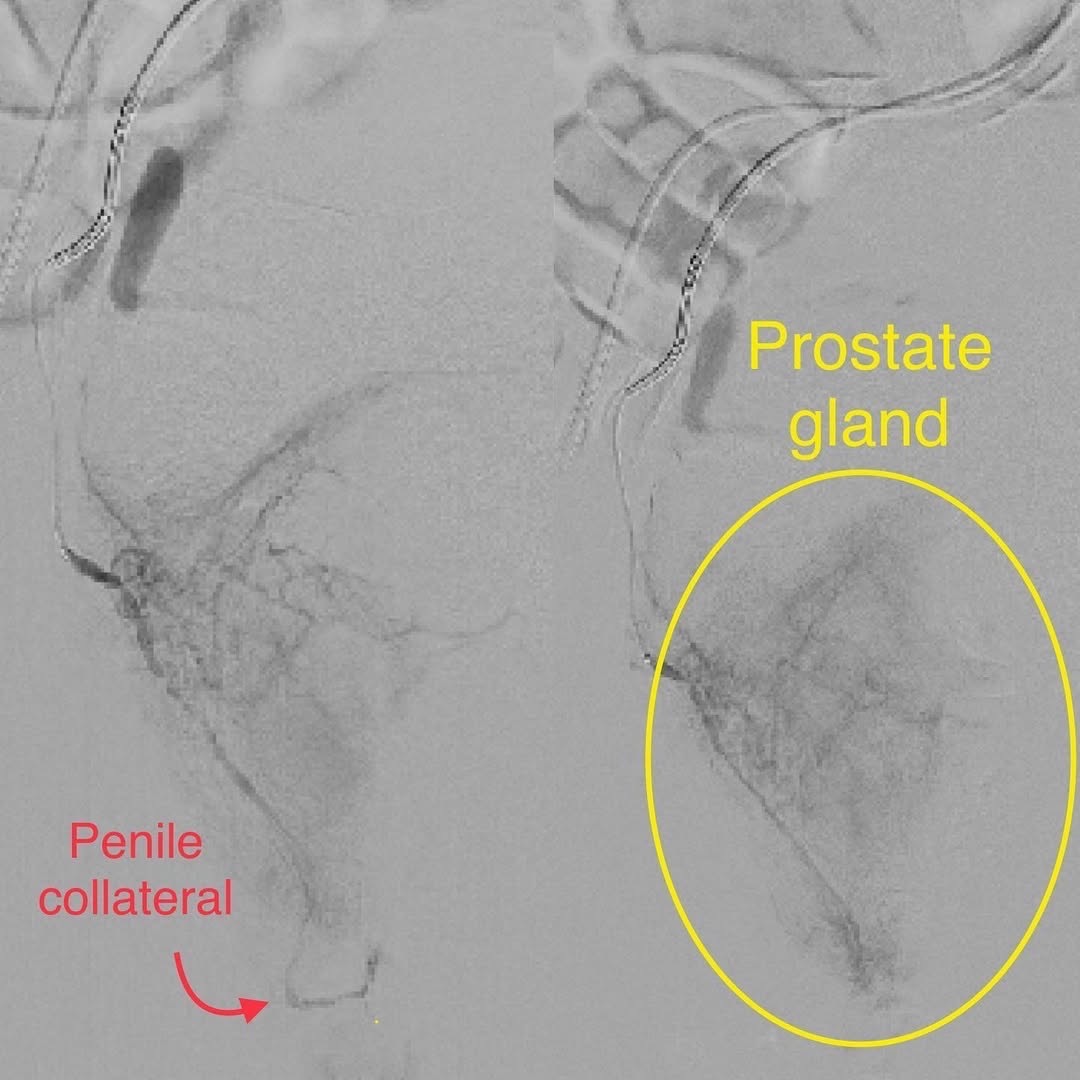
Pinpoint the prostate arteries
Embolize & go home
How effective is prostate artery embolization?
Published studies report 75–85% of men have significant improvement in urinary symptoms after PAE, with relief often beginning within weeks.
The benefits are durable, too: some studies report symptom improvement lasting up to six years after the procedure.6
Honest framing: long-term head-to-head studies of PAE vs. TURP are still ongoing. Short- to medium-term PAE results are very promising, while TURP remains the gold standard for long-term durability. The right choice depends on your prostate size, anatomy, and goals — which is exactly what a consultation sorts out.
What are the risks of PAE?
PAE has a favorable safety profile, but like any procedure it has risks — most are mild and short-lived.
- Post-embolization syndrome — mild pelvic pain, low-grade fever, or urinary symptoms in the first few days, which usually resolve on their own.
- Non-target embolization — a small risk that particles affect nearby vessels (e.g. bladder or rectum); minimized by an experienced operator.9
- Incomplete symptom relief — some men may need additional treatment.
- Technical demand — prostate artery anatomy varies between men, so PAE should be done by a highly skilled interventional radiologist.10
This is a procedure where operator experience matters a great deal. Choosing an interventional radiologist who performs PAE regularly is one of the most important factors in a safe, successful result.

How does PAE compare with TURP surgery?
PAE offers a less invasive option with comparable symptom relief, faster recovery, and far lower sexual side effects — while TURP remains the long-term durability benchmark.
PAE
- Needle puncture — no surgical cutting
- Local anesthesia and light sedation
- Outpatient — home the same day
- Quicker recovery, fewer limitations
- Much lower risk of sexual side effects
- Lower bleeding risk
TURP
- Surgical resection of prostate tissue
- Often regional or general anesthesia
- Usually requires a hospital stay
- Longer recovery
- Retrograde ejaculation up to 65%; ED up to 10%
- Notable bleeding risk
| Feature | PAE | TURP |
|---|---|---|
| Invasiveness | Minimally invasive (needle) | Surgical resection |
| Anesthesia | Local + light sedation | Regional or general |
| Setting | Outpatient, same-day | Usually hospital stay |
| Recovery | Quicker | Longer |
| Sexual side effects | Much lower | Higher (retrograde ejaculation, ED) |
| Long-term durability | Promising (studies ongoing) | Gold standard |
Who is a good candidate for PAE?
PAE is especially valuable for men with moderate-to-severe BPH, those who want to preserve sexual function, and those with very large prostates where surgery is riskier.
PAE is particularly beneficial for men who:
- Have moderate-to-severe BPH symptoms
- Are poor surgical candidates due to other health issues
- Want to preserve sexual function
- Have large prostates (over 80–100 grams), where TURP becomes less effective or riskier
Request an Appointment
Please note that although we strive to protect and secure our online communications, and use the security measures detailed in our Privacy Policy to protect your information, no data transmitted over the Internet can be guaranteed to be completely secure and no security measures are perfect or impenetrable. If you would like to transmit sensitive information to us, please contact us, without including the sensitive information, to arrange a more secure means of communication.
Who performs PAE at CVI Prostate Center?
At CVI Prostate Center, prostate artery embolization is performed by Dr. Atabak Allaei, a board-certified vascular and interventional radiologist with extensive experience in image-guided embolization. Because PAE is technically demanding and depends heavily on operator skill, your procedure is performed by the physician — not an assistant or non-physician provider — with careful patient selection and individualized planning.
Atabak Allaei, MD
Double board-certified in Vascular & Interventional Radiology and Diagnostic Radiology by the American Board of Radiology, with sub-specialty fellowship training and a proven track record of more than 5,000 image-guided procedures.
Prostate embolization: common questions
What is prostate artery embolization (PAE)?
Prostate artery embolization (PAE) is a minimally invasive, image-guided procedure for an enlarged prostate (BPH). An interventional radiologist guides a thin catheter to the arteries supplying the prostate and injects tiny particles to reduce its blood flow, causing the gland to shrink over the following weeks and relieving urinary symptoms — without surgery, cutting, or general anesthesia.
How effective is prostate artery embolization?
Clinical studies report that roughly 75–85% of men experience significant improvement in urinary symptoms after PAE. Prostate volume reductions of 20–40% are common, relief often begins within weeks, and some studies report benefits lasting up to six years.
Is PAE better than TURP surgery?
PAE and TURP are different tools. PAE is minimally invasive, outpatient, uses local anesthesia, has a quicker recovery, and a much lower risk of sexual side effects such as retrograde ejaculation. TURP remains the long-term gold standard for durability. The best choice depends on prostate size, anatomy, and individual goals — see our PAE vs. TURP comparison and discuss it at a consultation.
Does PAE affect sexual function?
PAE has much lower rates of sexual side effects than TURP. TURP is associated with retrograde ejaculation in up to 65% of men and erectile dysfunction in up to 10%; PAE preserves both ejaculation and erectile function in most cases, which is a key reason men choose it.
What is recovery like after PAE?
PAE is an outpatient procedure and most men go home the same day. Recovery is usually quick with fewer activity limitations than surgery. Some men experience mild pelvic discomfort, low-grade fever, or temporary urinary symptoms in the first few days — known as post-embolization syndrome — which typically resolves on its own.
Who is a good candidate for PAE?
PAE is well suited to men with moderate-to-severe BPH symptoms, those who are poor surgical candidates due to other health issues, men who want to preserve sexual function, and those with very large prostates (over 80–100 grams) where TURP becomes less effective or riskier. Men with severe bladder dysfunction or prostate cancer are typically not candidates.
What are the risks of prostate artery embolization?
PAE has a favorable safety profile. Possible risks include post-embolization syndrome (mild pelvic pain, low-grade fever, urinary symptoms for a few days), a small risk of non-target embolization affecting nearby structures, and incomplete symptom relief in some patients. Because prostate artery anatomy is variable, PAE is technically demanding and should be performed by an experienced interventional radiologist.
Is prostate artery embolization covered by insurance?
PAE is performed in California by our board-certified interventional radiologist, and appointments are available in person in Los Angeles, Orange County, and San Diego, or by video telehealth. Coverage varies by plan; our team can review your insurance and benefits when you request a consultation.
Explore prostate embolization further
PAE vs. TURP
A detailed side-by-side of the two procedures.
Our Specialist
Meet the board-certified IR who performs your PAE.
PAE & Insurance
How coverage works and what to expect.
What is Interventional Radiology?
The specialty behind image-guided treatment.
Find a Location
Los Angeles, Orange County & San Diego.
Our Difference
What sets our PAE program apart.
See if PAE is right for you
An enlarged prostate doesn’t have to mean surgery. Request a consultation and our board-certified interventional radiologist will review your imaging, labs, and history to determine whether you’re a candidate and what results to expect. Telehealth and in-person visits available across Los Angeles, Orange County and San Diego.



{kind=link}
{kind=link}